
Understanding DSM-5 acute stress disorder (ASD) is important for clinicians, students, and healthcare teams who work with people exposed to trauma. Acute stress disorder develops after a traumatic event and is an early mental health response to extreme stress. Symptoms can appear quickly and may include intense fear, dissociation, sleep problems, emotional numbness, and intrusive, distressing memories.
Using the DSM-5 criteria helps ensure accurate and consistent diagnosis. It also helps clinicians tell ASD apart from other trauma-related conditions, such as post-traumatic stress disorder (PTSD). This distinction matters because early identification and treatment can lower the risk of developing PTSD.
This guide offers a clear overview of ASD, including diagnostic criteria, symptom types, developmental and cultural factors, assessment tools, and evidence-based treatment options.
Understanding Acute Stress Disorder
Acute stress disorder (ASD) is classified in the Diagnostic and Statistical Manual as a stress disorder and acute trauma reaction that occurs shortly after a traumatic event. It is not a typical response to everyday stress. Instead, ASD reflects changes in emotional regulation, memory processing, and nervous system functioning following trauma.
What Defines Acute Stress Disorder?
According to the DSM-5, acute stress disorder requires exposure to a traumatic event involving:
- Actual or threatened death
- Serious injury
- Sexual violence
Exposure may occur through:
- Directly experiencing the trauma
- Witnessing the event
- Learning that a close family member or friend experienced trauma
- Repeated or extreme exposure to traumatic details as part of professional duties
Everyday stressors, even when overwhelming, do not meet the criteria for ASD.
Why Timing Matters
Timing is a key part of diagnosing acute stress disorder:
- Symptoms begin within days after the traumatic event
- Symptoms last from 3 days to 1 month
If symptoms continue beyond one month, clinicians must reassess the individual for post-traumatic stress disorder or another trauma-related condition.
The Role of DSM-5 in Diagnosis
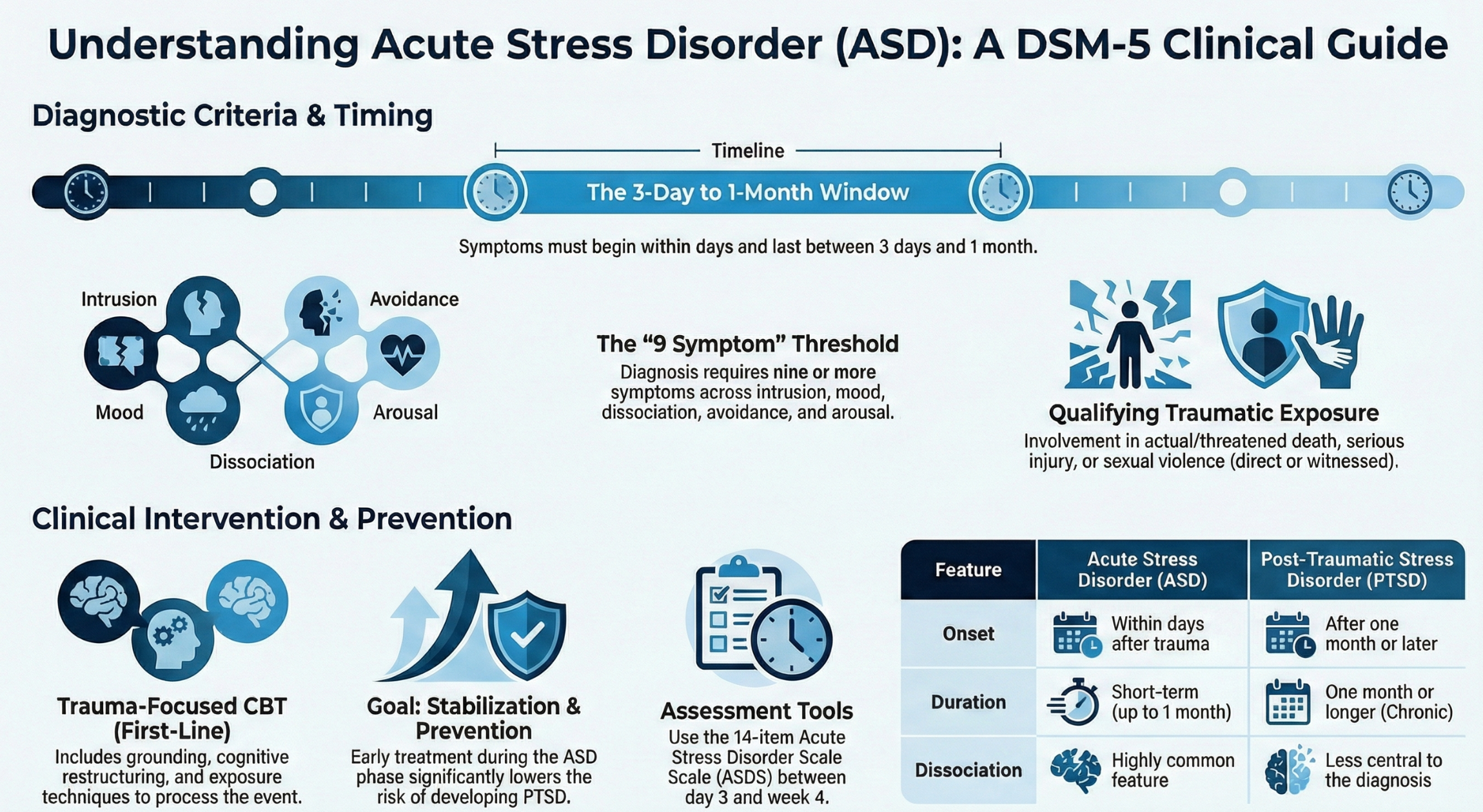
The DSM-5 gives clinicians a clear and consistent way to diagnose trauma-related conditions. For acute stress disorder (ASD), symptoms are grouped into five main areas: intrusion, negative mood, dissociation, avoidance, and arousal.
Instead of needing symptoms from specific groups, the DSM-5 uses a total symptom count. This approach allows flexibility while still keeping the diagnosis accurate.
DSM-5 Diagnostic Requirements
To diagnose acute stress disorder (ASD), all of the following must be true:
- The person was exposed to a traumatic event
- Nine or more symptoms are present from the DSM-5 list
- Symptoms cause clear distress or problems with daily functioning
- Symptoms begin and last between 3 days and 1 month after the trauma
- Symptoms are not better explained by substances, medical conditions, or another mental health disorder
This structured approach helps clinicians make accurate diagnoses while avoiding confusion with normal stress reactions.
Detailed Symptom Criteria for DSM-5 Acute Stress Disorder
The following sections explain how symptoms appear in real-world clinical practice.
Exposure to a Traumatic Event: What Counts
A qualifying trauma involves serious threat or harm. Clinicians should clearly note:
- How the person was exposed (directly, by witnessing, or by learning about it)
- The person’s relationship to the victim if the exposure was indirect
- Whether any media exposure was work-related
Media exposure does not qualify unless it is part of professional duties, such as for first responders, emergency clinicians, or investigators who are regularly exposed to graphic material.
Intrusion Symptoms
Intrusion symptoms involve unwanted and repeated thoughts or memories of the trauma. These symptoms show that the brain is having trouble processing the event.
Common examples include:
- Repeated intrusive memories
- Distressing dreams related to the trauma
- Flashbacks where the person feels the event is happening again
- Strong emotional or physical reactions to reminders
These symptoms are not intentional and often interfere with sleep, focus, and daily activities.
Negative Mood Symptoms
Negative mood in acute stress disorder is different from normal sadness. It means the person has trouble feeling positive emotions after the trauma.
People may report:
- Feeling emotionally numb
- Feeling unable to enjoy things they once liked
- Feeling disconnected from happiness
- Saying things like “I feel empty”
This reflects trauma-related changes rather than depression alone.
Dissociative Symptoms
Dissociation is a common part of acute stress reactions and may be hard to notice.
Signs may include:
- Feeling that the world is not real
- Feeling detached from oneself
- Trouble remembering important parts of the trauma
Dissociation can help protect the person at first, but it becomes a problem when it affects memory or daily life.
Avoidance Symptoms
Avoidance means trying to stay away from reminders of the trauma, such as:
- Avoiding thoughts or memories about the event
- Avoiding people, places, or situations linked to the trauma
While avoidance may reduce anxiety for a short time, it often keeps symptoms going.
Arousal Symptoms
Arousal symptoms show that the nervous system is on high alert after trauma. These may include:
- Sleep problems or insomnia
- Irritability or angry outbursts
- Being overly alert or watchful
- Strong startle reactions
- Trouble concentrating
Together, these symptoms reflect the typical ASD pattern of intrusion, negative mood, dissociation, avoidance, and arousal.
Duration and Symptom Thresholds
To diagnose acute stress disorder, clinicians must confirm that:
- Symptoms began or became worse after the traumatic event
- At least nine symptoms are present
- Symptoms occur within the acute time period
If symptoms last longer than one month, the person should be reassessed for post-traumatic stress disorder, which has different diagnostic criteria.
Acute Stress Disorder vs Posttraumatic Stress Disorder
Understanding the difference between ASD and PTSD helps guide monitoring and treatment planning.
| Feature | Acute Stress Disorder | Posttraumatic Stress Disorder |
|---|---|---|
| Onset | Within days after trauma | After one month or later |
| Duration | Short-term | One month or longer |
| Dissociation | Common | Less central |
| Risk | May resolve or progress | Often chronic |
Early intervention during ASD can prevent subsequent development of PTSD.
Developmental and Cultural Considerations
Children and Adolescents
In children, stress reaction include behavioral changes rather than verbal reports:
- Trauma-related play
- Regression in sleep or toileting
- Increased clinginess or irritability
Adolescents may show:
- Withdrawal
- Mood swings
- Risk-taking behaviors
Cultural Factors
Culture shapes how distress is expressed. Some individuals emphasize physical symptoms (headaches, stomach pain), while others interpret trauma reactions through spiritual or relational frameworks.
Clinicians should assess symptoms within cultural context to avoid misdiagnosis.
Practical Diagnostic Tools and Workflow
Acute Stress Disorder Scale (ASDS)
The ASDS is a 14-item self-report tool assessing:
- Intrusion
- Negative mood
- Dissociation
- Avoidance
- Arousal
It supports a stress disorder a systematic assessment approach when combined with clinical interviewing.
Best practices
- Use between day 3 and week 4 post-trauma
- Track symptom change over time
- Do not use as the sole diagnostic tool
Treatment of Acute Stress Disorder
Early Intervention Matters
The goal of treatment is symptom stabilization and prevention of PTSD.
Evidence-based treatments include:
- Trauma focused cognitive behavioral therapy
- Trauma focused CBT techniques such as grounding, exposure, and cognitive restructuring
- Psychoeducation about trauma responses
- Sleep and anxiety management strategies
Medication is not first-line but may be considered for severe anxiety or insomnia.
Early treatment reduces the need for long-term treatment of posttraumatic stress disorder PTSD.
Documentation and Follow-Up
Thorough documentation should include:
- Trauma exposure details
- Symptom examples with onset timing
- Functional impairment
- Planned reassessment at one month
Clear documentation improves continuity of care and diagnostic accuracy.
Final Thoughts
Acute stress disorder (ASD) represents a critical window for early intervention. When clinicians apply DSM-5 criteria, use structured assessment tools, and implement trauma-focused CBT, they can reduce distress, support stabilization, and lower the risk of long-term trauma complications such as post-traumatic stress disorder. Careful assessment, cultural sensitivity, and timely follow-up remain essential parts of effective trauma-informed care.
Recovery during the acute phase can also benefit from broader support that helps regulate stress, sleep, and emotional balance.
Take the Cenario Quiz to get personalized supplement recommendations tailored to your current needs. The quiz is designed to support stress response and overall well-being as part of a comprehensive recovery approach, alongside, not in place of, professional care.
Frequently Asked Questions
Can acute stress disorder go away on its own?
Yes, acute stress disorder (ASD) can improve on its own in some people, especially when symptoms are mild and short-lived. However, when symptoms are intense, involve dissociation, or interfere with daily life, early support is important. Timely assessment and early intervention can reduce distress and lower the risk of developing post-traumatic stress disorder (PTSD).
What is the recommended first-line treatment for acute stress disorder?
The first-line treatment for acute stress disorder is early trauma-focused cognitive behavioral therapy (CBT). This approach helps individuals process the traumatic event, reduce intrusive symptoms, manage avoidance, and calm heightened arousal. Supportive care, sleep stabilization, and stress-management strategies are often used alongside therapy.
How can individuals support recovery during the acute stress period?
Recovery from acute stress disorder involves more than symptom monitoring. Along with professional care, people may benefit from regular routines, adequate sleep, and stress-regulation techniques. Psychoeducation and supportive wellness strategies can complement clinical treatment and promote emotional balance during early recovery.