

A Comprehensive Guide to Understanding TF-CBT and Its Impact on Healing from Trauma
Trauma is not just a moment in time , it’s an experience that can ripple throughout every aspect of a person’s life, especially when it occurs during childhood or adolescence. When left unaddressed, trauma can lead to a cascade of emotional, psychological, and behavioral challenges that affect development, relationships, school performance, and overall quality of life.
But there is hope. Mental health professionals have developed effective, evidence-based treatments to support healing. Among the most successful of these is Trauma-Focused Cognitive Behavioral Therapy (TF-CBT), a structured, short-term, and highly effective treatment model specifically designed for young people dealing with the aftermath of trauma.
In this blog post, we’ll take a deep dive into the principles, process, and power of TF-CBT, helping you understand what it is, how it works, and how it helps children and families move toward recovery.
What is Trauma-Focused Cognitive Behavioral Therapy (TF-CBT)?
TF-CBT is a therapeutic intervention model developed to address the complex needs of children (ages 3–18) who have experienced trauma and are suffering from emotional or psychological distress as a result. It is rooted in the principles of traditional Cognitive Behavioral Therapy (CBT), which focuses on identifying and changing harmful thought patterns and behaviors. TF-CBT expands on this by incorporating trauma-sensitive strategies, psychoeducation, and a strong emphasis on caregiver involvement.
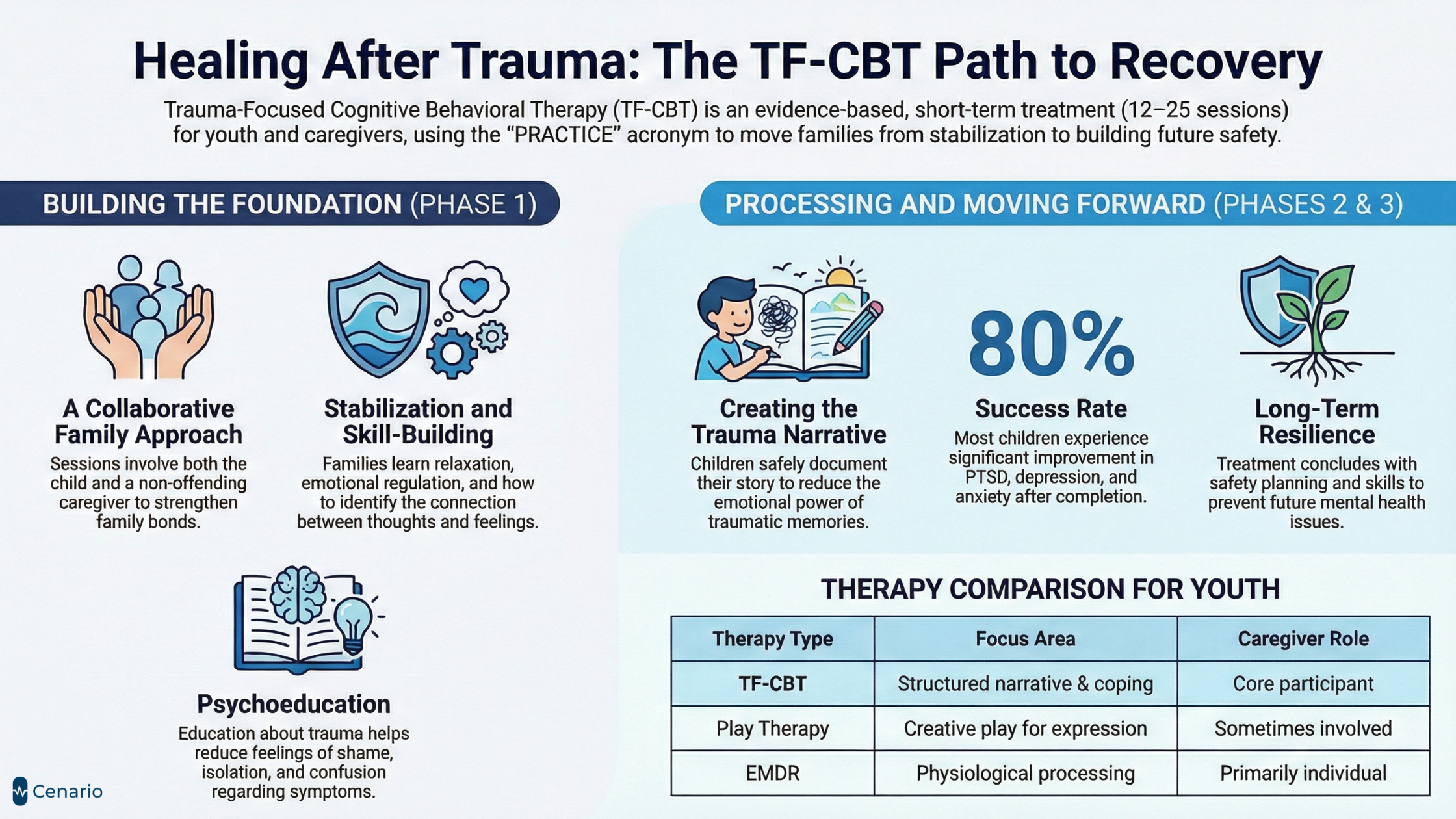
TF-CBT is highly structured and goal-oriented, typically delivered over the course of 12 to 25 weekly sessions, depending on the needs of the child. Sessions involve both the child and a non-offending caregiver, allowing for collaborative healing, improved communication, and strengthened family bonds.
What Kinds of Trauma Can TF-CBT Address?
TF-CBT is suitable for children and teens who have experienced a wide range of traumatic events, including:
- Sexual abuse or assault
- Physical abuse or neglect
- Exposure to domestic violence
- Sudden or traumatic death of a loved one
- Natural disasters (earthquakes, floods, fires)
- Serious accidents or injuries
- Community or school violence
- Refugee trauma or war-related displacement
- Medical trauma (e.g., hospitalization, chronic illness)
The therapy is also effective for children dealing with complex trauma, where multiple or repeated traumas have occurred over time.
Why Is TF-CBT Different From Regular CBT?
While traditional CBT focuses on changing unhelpful thoughts and behaviors, TF-CBT addresses the unique challenges associated with traumatic experiences, especially in children. These differences include:
- A developmentally appropriate approach for children and teens
- Inclusion of caregivers or parents in the healing process
- Emphasis on processing traumatic memories safely
- Addressing trauma-related guilt, shame, avoidance, and fear
- Focus on building resilience and future safety
TF-CBT is specifically structured to allow for gradual exposure to trauma-related memories and triggers in a controlled and supportive setting.
The 3 Phases of TF-CBT Treatment
TF-CBT follows a structured model known by the acronym PRACTICE, broken down into three distinct phases:
Phase 1: Stabilization and Skill-Building (Sessions 1–8)
The initial phase helps the child and caregiver develop the tools needed for emotional regulation and safety. This lays the foundation for deeper trauma processing later on.
Components:
-
Psychoeducation
- Educating the child and caregiver about trauma, common reactions, and the treatment process.
- Helps reduce feelings of shame, isolation, or confusion about trauma-related symptoms.
-
Parenting Skills
- Caregivers are taught behavior management techniques and supportive parenting strategies.
- Enhances the parent-child relationship and provides caregivers with tools to respond effectively to trauma symptoms.
-
Relaxation Techniques
Children learn calming skills like:
- Deep breathing
- Progressive muscle relaxation
- Visualization
- Mindfulness exercises
- Helps regulate physical responses to stress.
-
Affective Expression and Regulation
- Children learn to identify and express emotions in healthy ways.
- Therapists help expand emotional vocabulary, increase emotional awareness, and develop coping strategies.
-
Cognitive Coping Skills
- Children are taught the connection between thoughts, feelings, and behaviors.
- They practice identifying negative or distorted thoughts and replacing them with balanced, helpful thoughts.
Phase 2: Trauma Narration and Cognitive Processing (Sessions 9–16)
This is often the most emotionally intense and transformative part of TF-CBT. It involves facing the trauma in a structured and safe way, helping to reduce its emotional power.
Components:
-
Trauma Narrative Development
- The child creates a detailed narrative of the traumatic experience (verbally, written, or through creative expression).
- This gradual exposure helps reduce fear and avoidance of the memory.
- The therapist helps the child integrate the memory into their life story without being overwhelmed by it.
-
Cognitive Processing of the Trauma
- Therapists help children challenge inaccurate beliefs (e.g., “It was my fault,” or “I’m permanently damaged”).
- This helps reframe the trauma in a more realistic and empowering light.
Phase 3: Integration and Consolidation (Sessions 17–25)
In the final phase, the therapist helps the child and caregiver move forward, using the skills and insights gained in therapy to build a safe, fulfilling future.
Components:
-
In Vivo Exposure (as needed)
- Gradual, supported exposure to trauma reminders in real life (e.g., visiting a location, hearing a sound, or wearing certain clothes).
- This is done only when avoidance is impairing daily functioning.
-
Conjoint Parent-Child Sessions
- Children and caregivers meet together to discuss the trauma narrative, share feelings, and support each other.
- This phase fosters open communication, trust, and healing within the family system.
-
Enhancing Safety and Future Development
Focuses on:
- Creating a personal safety plan
- Identifying risk factors
- Teaching assertiveness and problem-solving skills
- Emphasizes preparing the child for a trauma-free future.
Who Is TF-CBT Best Suited For?
TF-CBT is most effective for:
- Children and adolescents (ages 3–18)
- Those experiencing PTSD, depression, anxiety, or behavioral issues following trauma
- Families willing to actively participate in therapy
It is NOT suitable for:
- Situations where the caregiver is the perpetrator and not removed from the environment
- Families who are unwilling to engage in treatment
- Children with active psychosis or severe developmental delays (unless modified)
Evidence of Effectiveness
TF-CBT is one of the most studied and evidence-supported interventions for childhood trauma.
Research findings show:
80%+ of children experience significant improvement after completing TF-CBT
Reduction in:
- PTSD symptoms
- Depression and anxiety
- Behavioral outbursts
- Shame and guilt
Caregivers report:
- Better parenting skills
- Improved communication with their child
- Reduction in their own distress
TF-CBT has been successfully implemented across different cultures, languages, and settings — including schools, hospitals, foster care systems, refugee programs, and community mental health centers.
What to Expect in a TF-CBT Session
- Sessions typically last 45 to 60 minutes
- Therapy occurs once per week
The therapist will alternate between:
- Individual sessions with the child
- Individual sessions with the caregiver
- Joint sessions with both
Activities include:
- Talking
- Drawing or creative expression
- Role-playing
- Practicing skills
Therapists follow the PRACTICE model but remain flexible and responsive to the needs and pace of the child.
The Role of the Therapist
A TF-CBT therapist is:
- Specially trained in trauma and child development
- Compassionate, culturally sensitive, and non-judgmental
- Skilled in creating a safe, structured, and engaging environment
- A partner to both the child and caregiver throughout the healing process
Benefits of TF-CBT
- Faster recovery compared to unstructured therapy
- Long-term emotional resilience
- Strengthened parent-child relationships
- Reduced reliance on medication
- Prevention of future mental health issues
TF-CBT vs. Other Trauma Therapies: How Does It Compare?
When exploring therapy options for a child who has experienced trauma, parents and caregivers may feel overwhelmed by the different methods available. While TF-CBT is one of the most effective and evidence-backed approaches, it’s helpful to understand how it compares to other trauma-focused therapies. Each approach has unique techniques, benefits, and target populations.
Here’s a detailed breakdown:
| Therapy Type | Description | Best For | Caregiver Involvement | Structure & Length |
|---|---|---|---|---|
| TF-CBT (Trauma-Focused Cognitive Behavioral Therapy) | Structured, short-term therapy that uses CBT principles tailored to trauma. Includes a trauma narrative, relaxation skills, and joint caregiver sessions. | Children/adolescents (ages 3–18) experiencing PTSD, abuse, grief, or complex trauma | Yes – core part of treatment | 12–25 sessions, structured format |
| EMDR (Eye Movement Desensitization and Reprocessing) | Uses bilateral stimulation (eye movements or tapping) to reduce distress associated with trauma memories. | Individuals with single-event trauma; adults or older children | No – primarily individual-focused | Varies (6–20+ sessions) |
| Play Therapy | Non-directive or directive therapy using toys and creative play to help children express feelings and process trauma. | Young children (typically 3–10) | Sometimes | Ongoing or open-ended |
| Narrative Therapy | Focuses on helping individuals “re-author” their life stories by separating themselves from their problems. Encourages empowerment and redefinition of identity. | Older children, teens, and adults with complex or identity-related trauma | Optional | Open-ended; flexible structure |
| DBT (Dialectical Behavior Therapy) | Combines CBT with mindfulness and emotional regulation strategies; originally developed for borderline personality disorder but now adapted for trauma. | Teens with self-harm, emotional dysregulation, suicidal ideation | Limited; usually individual-based | 6+ months; skills training groups included |
Key Differences:
- TF-CBT is uniquely designed for children with trauma, integrating caregiver support, emotional skill-building, and trauma processing techniques.
- EMDR is more passive in that it focuses less on narrative or talking and more on physiological processing.
- Play therapy is ideal for younger children who struggle with verbal expression.
- Narrative and DBT are more suitable for teens or adults and may be used as supplementary treatments after initial trauma stabilization.
Why Choose TF-CBT?
Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) stands out as one of the most effective treatments for childhood trauma, backed by over 20 years of rigorous clinical research. One of its greatest strengths is the inclusion of caregivers throughout the process, which significantly enhances treatment outcomes by creating a supportive and healing environment at home. TF-CBT not only helps children process traumatic experiences but also equips them with lifelong coping strategies and emotional resilience. Its structured yet flexible framework makes it highly adaptable to various types of trauma, including complex and chronic cases, ensuring that each child receives care tailored to their specific needs.
Real-Life Success Story (Case Example)
Stories are powerful tools for understanding the real-world impact of TF-CBT. While confidentiality laws prevent the use of real client identities, the following composite case example is based on real therapeutic principles and scenarios commonly seen in TF-CBT.
Case Example: “Liam, Age 12”
Background:
Liam, a 12-year-old boy, witnessed the violent death of his older brother during a drive-by shooting in their neighborhood — a traumatic event that deeply shook his sense of safety and stability. In the weeks and months that followed, Liam began showing signs of severe post-traumatic stress. He struggled with persistent nightmares and insomnia, became increasingly irritable, and experienced frequent anger outbursts at school. He avoided going outside, startled easily at sudden noises, and grew distant from friends and family members. His once bright and curious demeanor faded, and his parents grew concerned as he rarely spoke about what had happened and became increasingly withdrawn.
TF-CBT in Action
Sessions 1–5: Skill-Building & Stabilization
Liam learned relaxation strategies such as square breathing, muscle relaxation, and visual grounding techniques. He and his parents received psychoeducation about trauma and the brain — learning how Liam’s symptoms were a normal response to a terrifying event.
Sessions 6–10: Developing the Trauma Narrative
Using a graphic novel format, Liam slowly began writing and drawing his trauma story. With his therapist, he processed key moments such as the event itself, his feelings of survivor’s guilt, and thoughts like “It should have been me.”
Sessions 11–15: Conjoint Sessions with Parents
In joint sessions, Liam shared parts of his trauma narrative with his parents. His father cried for the first time in years, validating Liam’s feelings and saying, “You don’t have to carry this alone.” This moment marked a turning point in Liam’s healing.
Sessions 16–20: Safety Planning & Integration
Liam created a “future safety plan” with his parents and therapist, identifying safe routes to school, trusted adults, and peer supports. He rejoined the school basketball team and started sleeping better at night.
Outcome:
Over the course of treatment, Liam experienced a significant reduction in nightmares and sleep disturbances. He gradually reopened communication with his parents, expressing thoughts and feelings he had previously kept bottled up. With renewed confidence and emotional stability, he returned to school full-time and re-engaged with peers and learning. By the end of the therapy process, Liam no longer met the clinical criteria for PTSD. His story is a powerful example of the transformative potential of TF-CBT when caregivers, therapists, and children work together in a compassionate, structured, and supportive environment.
Cultural Considerations in TF-CBT
Trauma does not happen in a vacuum – it is shaped and understood through the cultural lens of the child and family. Effective TF-CBT implementation must consider:
1. Cultural Beliefs Around Mental Health
- In some cultures, trauma is not openly discussed, or emotional expression is discouraged.
- Therapy may be seen as shameful, private, or even unnecessary.
Example: A family from a collectivist culture might believe discussing trauma brings shame to the entire family unit. A TF-CBT therapist may adapt by using metaphors and symbols relevant to the family’s traditions to approach the topic respectfully.
2. Spiritual and Religious Beliefs
- Children and caregivers may attribute trauma to spiritual causes (e.g., punishment, karma, divine intervention).
- A culturally attuned therapist will respect these views and integrate them into the healing process when appropriate.
Example: A child from a religious background may include prayer or scripture as part of their coping plan.
3. Language and Communication Styles
- TF-CBT can be adapted with translators or bilingual therapists.
- Some cultures rely more on nonverbal communication (e.g., storytelling, body language), which can be incorporated into the trauma narrative process.
4. Family Structure and Roles
- In some cultures, extended family or elders play a vital role in child-rearing.
- Therapists may invite broader family involvement to reflect cultural values and strengthen support.
Cultural Responsiveness in TF-CBT Means:
- Avoiding one-size-fits-all approaches
- Asking open-ended, respectful questions about cultural practices
- Adjusting strategies to align with client worldviews
- Being aware of one’s own biases and assumptions
Barriers to Accessing TF-CBT
Even though TF-CBT is effective, many families face significant challenges in accessing it. Understanding and addressing these barriers is essential for improving mental health equity.
Common Barriers:
Limited Availability of Trained Providers
- Not all therapists are certified or trained in TF-CBT.
- Rural or underserved areas often lack child-focused mental health services.
Financial Constraints
- High costs for therapy (especially without insurance).
- Medicaid and public programs may not always cover specialized treatments.
Stigma and Misconceptions
- Cultural or religious beliefs may discourage seeking therapy.
- Fear of being labeled “mentally ill” or “broken.”
Language and Communication Barriers
- Limited access to bilingual therapists.
- Difficulty expressing trauma in a second language.
Lack of Transportation or Childcare
Getting to appointments can be difficult, especially for working parents.
Solutions and Workarounds:
- Telehealth / Online TF-CBT: Remote therapy using secure video platforms (increasingly covered by insurance)
- School-based TF-CBT programs: On-site support in schools or partnerships with school counselors
- Sliding scale clinics: Nonprofits and university clinics offering therapy based on income
- Community outreach: Culturally competent education campaigns to normalize therapy
Role of Schools and Educators in TF-CBT Support
Schools are often the first environments where trauma symptoms become visible, and educators can play a critical role in both identifying and supporting children in therapy.
How Educators Can Support TF-CBT:
Early Identification
- Recognize behavioral signs: hyperactivity, aggression, avoidance, perfectionism, dissociation
- Refer students to school counselors or mental health providers when concerns arise
Creating Trauma-Informed Classrooms
- Predictable routines help reduce anxiety
- Use of calm-down corners, break passes, and visual schedules
- Avoiding punishment for trauma-related behaviors (e.g., zoning out)
Collaborating with Therapists
With caregiver consent, therapists can:
- Share coping tools to use in class
- Provide trauma-informed classroom strategies
- Keep educators updated on progress (without breaching confidentiality)
Peer Support and Inclusion
- Encouraging peer relationships and group activities to rebuild trust
- Preventing bullying or isolation
Professional Training for Teachers
- Workshops on trauma-informed care
- Learning to de-escalate crisis moments with empathy and structure
Why School Collaboration Matters
- Children spend 6–8 hours per day in school
- Educators often have consistent, long-term contact with children
- Supportive school environments reinforce what is learned in TF-CBT sessions

Final Thoughts: The Path to Healing Through TF-CBT
Trauma can profoundly affect a child’s development, identity, and relationships, but it doesn’t have to define their future. Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) offers a structured, supportive, and proven path to recovery, giving children the tools to process what they’ve experienced and build resilience for life.
What sets TF-CBT apart is its whole-family approach, blending evidence-based techniques with compassion, cultural sensitivity, and real-world applicability. It doesn’t just treat symptoms, it empowers children and caregivers to move forward together, with confidence and hope.
If you or someone you know is navigating the aftermath of trauma, don’t wait. Reach out to a licensed TF-CBT therapist and take the first step toward healing. The effects of trauma are real, but so is recovery.
Looking for Additional Support Alongside Therapy?
Sometimes, healing from trauma also means supporting the body and mind beyond therapy sessions, through better sleep, reduced anxiety, stronger focus, and emotional balance.
Take the Cenario Quiz to receive personalized supplement recommendations tailored to your mental wellness needs. Whether you or your child are dealing with sleep issues, emotional overwhelm, or focus difficulties, the Cenario quiz will guide you to safe, science-backed supplements that support healing from the inside out.
Take the Cenario Quiz now https://cenario.com/quiz/and discover custom support options designed just for you or your child.
Because every trauma journey is unique – and so is your recovery.
Frequently Asked Questions (FAQs) About TF-CBT
Frequently Asked Questions
1. Will TF-CBT re-traumatize my child by making them talk about painful experiences?
This is one of the most common concerns among caregivers, and an understandable one. However, TF-CBT is carefully designed to prevent re-traumatization.
Rather than diving straight into painful memories, therapy begins with emotional safety, skill-building, and trust. Children learn relaxation techniques, emotional regulation, and coping tools before discussing their trauma. The trauma narrative portion only begins once the child is ready, and even then, it is introduced gradually and at the child’s pace.
Therapists are trained to recognize signs of distress and will never force a child to disclose more than they feel comfortable sharing. The goal is not to relive the trauma, but to gain control over it and reduce its emotional power.
2. What if my child refuses to talk about the trauma or doesn’t want to go to therapy?
It’s very common for children to feel hesitant, scared, or even resistant to therapy, especially when trauma is involved. However, TF-CBT therapists are trained to engage children in creative, non-threatening ways, such as:
- Drawing or writing
- Role-play or storytelling
- Art and games
- Building a trusting relationship first
In the early sessions, the therapist focuses on building rapport and teaching helpful skills rather than jumping into deep topics. As the child begins to feel safer, they often become more open to discussing their experiences.
Additionally, involving a trusted non-offending caregiver helps tremendously. Children feel more supported and less alone when their parent or guardian is part of the process.
3. Can TF-CBT be done online or through telehealth? Is it just as effective?
Yes, TF-CBT can be effectively delivered via telehealth, and many providers began offering remote sessions during the COVID-19 pandemic with excellent outcomes.
Online TF-CBT follows the same structure as in-person therapy, with the same PRACTICE components. Therapists use interactive tools, digital worksheets, and video conferencing platforms to maintain engagement.
Research supports the effectiveness of online TF-CBT, especially when:
- The child has a private, quiet space for sessions
- The caregiver is involved and present
- The therapist is trained in telehealth delivery
It’s a valuable option for families in rural areas, during transportation challenges, or where in-person therapy isn’t accessible.
4. What is the role of the caregiver in TF-CBT, and what if I don’t feel equipped to help?
In TF-CBT, the caregiver plays a vital and active role in the healing process. Far from needing to be an expert, what’s most important is your presence, support, and willingness to participate.
The therapist will teach you parenting skills, provide trauma education, and involve you in sessions so you can:
- Understand your child’s behavior
- Respond in emotionally supportive ways
- Help reinforce skills outside therapy
- Process your own feelings related to the trauma
Many caregivers also experience guilt, anger, or confusion about the trauma. TF-CBT provides space for you to heal, too, while supporting your child.
If you’re feeling overwhelmed, know this: you don’t need to have all the answers — just showing up makes a difference.
5. How long does TF-CBT take, and how soon will I see results?
TF-CBT is considered a short-term therapy, typically lasting 12 to 25 weekly sessions, depending on the child’s needs, the complexity of the trauma, and how quickly progress is made.
While each case is unique, many families begin noticing changes within the first 4–6 sessions, including:
- Fewer nightmares or sleep issues
- Improved mood or fewer tantrums
- Greater communication between parent and child
- Better coping when faced with reminders of the trauma
The therapy is structured in three phases, so parents can track progress along the way. The ultimate goal is not only symptom reduction but long-term emotional resilience and stability.
6. Is TF-CBT covered by insurance or Medicaid? How do I find a certified therapist?
Yes, TF-CBT is widely covered by health insurance plans, including Medicaid, depending on your state and provider network. Many community mental health centers, children’s hospitals, and nonprofit organizations offer TF-CBT either free of charge or on a sliding scale based on income.
To find a qualified provider:
- Visit the official TF-CBT therapist registry
- Use trusted directories like Psychology Today, GoodTherapy, or your local mental health department
- Ask your pediatrician, school counselor, or social worker for referrals
- Look for therapists who are TF-CBT certified or trained, licensed, and experienced with children or adolescents
If you need help navigating insurance or referrals, many clinics have intake coordinators who can walk you through the process.





