

What Fatal Insomnia Is
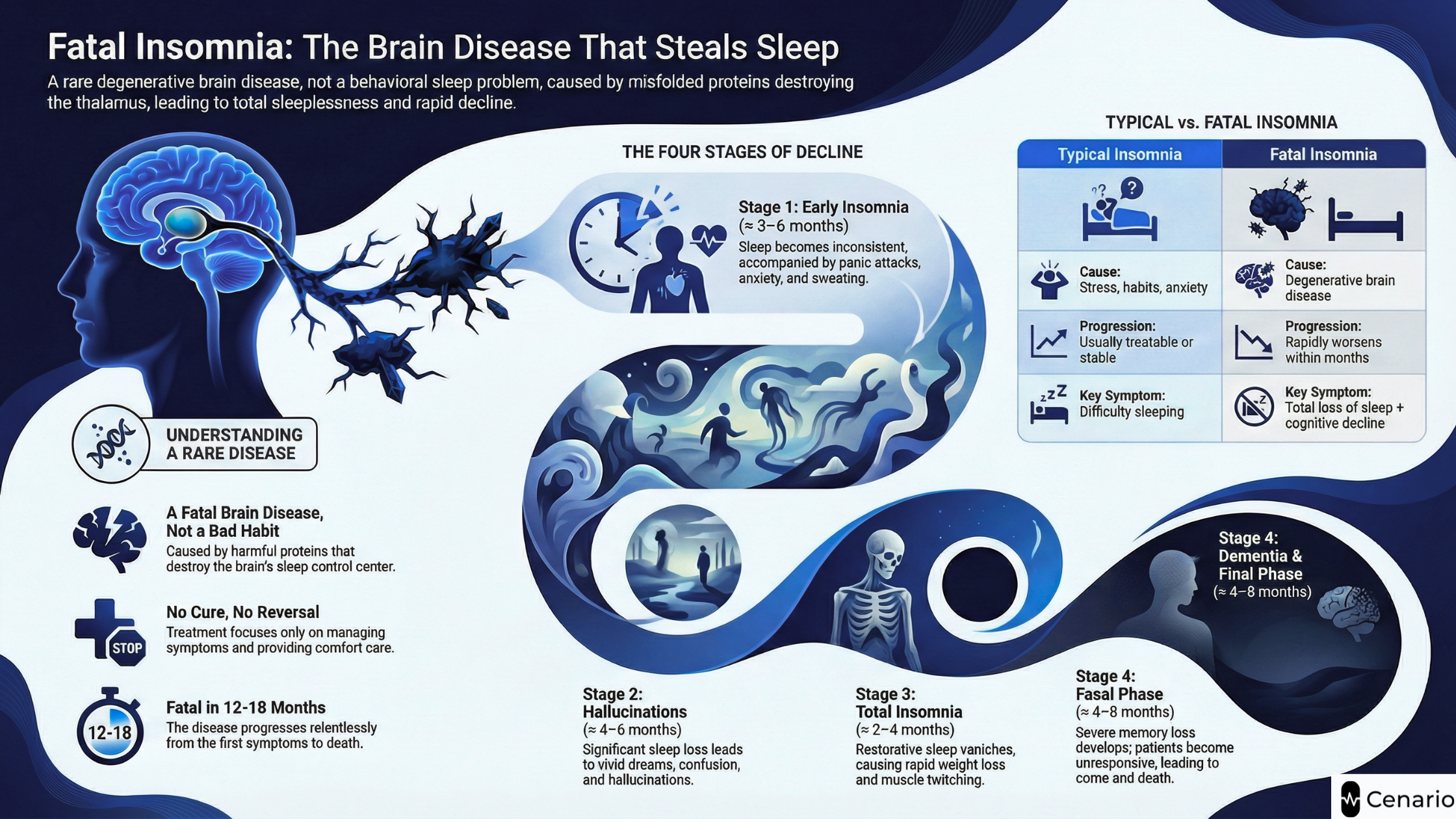
Fatal insomnia is one of the rarest and most serious sleep disorders in the world. Unlike regular insomnia caused by stress, anxiety, or poor sleep habits, fatal insomnia is a degenerative brain disease. It affects the thalamus, the part of the brain that controls the sleep, wake cycle and important body functions such as blood pressure, heart rate, and temperature. As the disease gets worse, a person slowly loses the ability to sleep at all. This leads to rapid physical and mental decline.
There are two types of fatal insomnia. Fatal Familial Insomnia (FFI) is inherited and runs in families. Sporadic Fatal Insomnia (SFI) does not come from a family history and appears unexpectedly. Even though they start differently, both types damage the brain in the same way.
What Fatal Insomnia Is
Fatal insomnia happens when a normal protein in the body, called PrPC, changes into a harmful form known as PrPSc. The body cannot remove this damaged protein, so it builds up in the brain and kills nerve cells. In FFI, this process is caused by a mutation in the PRNP gene, most commonly the D178N mutation. SFI appears without a known genetic cause, but the same harmful protein changes still occur.
The thalamus is responsible for creating deep sleep, including slow-wave sleep and sleep spindles. When this area is damaged, the brain can no longer produce normal, restorative sleep. Over time, other parts of the brain that control memory, movement, and body functions also begin to fail.
How Fatal Insomnia Differs From Typical Insomnia
Most people experience insomnia because of stress, mental health concerns, or poor routines. This type of insomnia is uncomfortable but not dangerous, and it usually improves with treatment or lifestyle changes.
Fatal insomnia is very different because:
- It is caused by a brain disease, not habits or behavior.
- Sleep medications usually do not work.
- Symptoms get worse quickly, often within months.
- Problems with thinking, hallucinations, and body control appear early.
This rapid decline, combined with the complete loss of sleep—makes fatal insomnia extremely serious.
Why Awareness Matters
Fatal insomnia is extremely rare, but being aware of it helps families who may be at risk. Early recognition can lead to faster neurological evaluation, proper genetic testing, and early planning for care. Understanding the disease also helps caregivers prepare for the emotional and physical challenges ahead.
For simple explanations or help deciding when to see a specialist, you can check our dictionary entry or take the short risk quiz.
Pathophysiology and Causes
Fatal insomnia begins when prion proteins misfold and turn into the toxic form, PrPSc. These harmful proteins:
- build up in the thalamus
- cause inflammation
- kill nerve cells
- disrupt sleep, memory, and body functions
In FFI, the PRNP mutation makes this misfolding more likely. In SFI, the misfolding happens on its own. In both types, the damage to the thalamus prevents the brain from creating deep sleep. As a result, patients experience fragmented, non-restful sleep, severe fatigue, and worsening cognitive symptoms.
Problems with temperature control, sweating, heart rate, and blood pressure also occur because the damaged brain regions help regulate these functions
Sleep Studies and Imaging
Doctors use polysomnography, EEG, and brain imaging to support a diagnosis. These tests may show:
- marked loss of slow-wave sleep
- absence of sleep spindles and K-complexes
- irregular or chaotic transitions between sleep stages
- EEG patterns suggesting thalamic dysfunction
- FDG-PET scans showing lower metabolic activity in the thalamus
- MRI scans that appear normal early but show subtle changes later
These findings help distinguish fatal insomnia from psychiatric disorders, primary insomnia, or other neurological conditions.
Symptoms and Stage Progression
Fatal insomnia typically progresses through four stages, although the timeline varies between patients. The entire course usually lasts about 12–18 months.
Stage 1: Early Insomnia and Autonomic Overactivity (≈ 3–6 months)
Sleep becomes shallow and inconsistent. Anxiety, panic attacks, sweating, and a fast heart rate are common.
Stage 2: Hallucinations and Worsening Sleep Loss (≈ 4–6 months)
Patients may experience vivid dreams, hallucinations, confusion, and significant sleep disruption.
Stage 3: Near-Total Insomnia and Physical Decline (≈ 2–4 months)
Most restorative sleep disappears. People lose weight rapidly and experience tremors, muscle twitching (myoclonus), and blood pressure instability.
Stage 4: Cognitive Decline and Terminal Phase (≈ 4–8 months)
Severe memory loss and dementia develop. Patients often become mute or unresponsive. Autonomic failure eventually leads to coma and death.
This fast and relentless progression is a defining feature of fatal insomnia.
Epidemiology and Risk Factors
Fatal insomnia is extremely rare. Only a small number of families around the world carry the PRNP gene mutation that causes Fatal Familial Insomnia (FFI), and confirmed cases of Sporadic Fatal Insomnia (SFI) are even fewer. Most people develop symptoms between ages 40 and 60, although younger and older cases have been documented.
For individuals without a family history of FFI, the likelihood of developing fatal insomnia is extremely low. However, anyone who has relatives with unexplained, rapidly worsening sleep problems or cognitive decline may benefit from genetic counseling to better understand their risks.
Diagnosis and Evaluation
Diagnosing fatal insomnia requires several steps. Doctors begin with a detailed clinical evaluation, looking at how quickly the symptoms appeared and whether common sleep medications provide any relief. They also check for autonomic symptoms like excessive sweating, unstable blood pressure, and temperature changes, which often appear early in the disease.
Sleep studies (polysomnography) help confirm the loss of deep, restorative sleep. EEG tests and brain imaging can reveal abnormalities in the thalamus, the brain region most affected by fatal insomnia. In families with suspected FFI, PRNP gene testing provides a clear and definitive diagnosis.
Before diagnosing fatal insomnia, doctors must rule out more common causes of severe sleep disturbance, such as autoimmune disorders, infections, nutrient deficiencies, psychiatric illnesses, and side effects from medications.
Management and Treatment
There is currently no cure for fatal insomnia, and no treatment can slow its progression. Instead, care focuses on managing symptoms and keeping the patient as comfortable as possible. Doctors may adjust medications to avoid those that worsen confusion or autonomic instability. Sedatives or sleep-promoting drugs may be used, but they typically do not restore normal sleep patterns.
Supportive care plays a major role. This includes maintaining proper hydration and nutrition, stabilizing blood pressure and heart rate, managing muscle twitching, and ensuring safe mobility. The most effective care usually comes from a multidisciplinary team, which may include neurologists, sleep specialists, mental health professionals, pharmacists, and palliative care providers.
Prognosis and Support
Fatal insomnia is a progressive and fatal disease. Most patients survive between 12 and 18 months after symptoms begin. Because of its rapid progression, early involvement of palliative care is essential. Palliative teams help manage distressing symptoms, provide emotional support, and guide families through difficult decisions about feeding, hydration, and overall comfort.
Families affected by FFI should consider genetic counseling to understand how the disease is inherited, explore testing options for relatives, and plan for future family decisions. Caregivers also benefit from support services such as respite care, legal and financial guidance, and rare-disease support groups, which can help reduce stress and prevent burnout.
Final Thoughts
Fatal insomnia is incredibly rare but profoundly serious. Recognizing its symptoms, understanding its genetic risks, and knowing when to seek help can make an important difference for families facing this disease. If you or someone you know is experiencing rapidly worsening insomnia, hallucinations, cognitive decline, or severe autonomic symptoms, a neurological evaluation is essential.
Improve your sleep, mood, and daily energy with science-backed support.
Take the Cenario Quiz to find personalized supplements recommendations designed for your unique needs.
Frequently Asked Questions
Can fatal insomnia be cured or reversed?
No. At this time, there is no cure or treatment that can stop or reverse fatal insomnia. Because it is a prion disease, the misfolded proteins continue to damage the brain over time. Treatment focuses on symptom management, improving comfort, and providing supportive and palliative care.
How is fatal insomnia different from chronic insomnia?
Chronic insomnia is usually caused by stress, anxiety, lifestyle habits, or medical conditions. It can often be treated with therapy, sleep hygiene, or medication. Fatal insomnia is a degenerative brain disorder, not a behavioral issue. It progresses rapidly, does not respond to sleep medications, and causes cognitive decline, hallucinations, and autonomic problems.
Is fatal insomnia genetic?
Fatal Familial Insomnia (FFI) is genetic and caused by a mutation in the PRNP gene. It follows an autosomal dominant inheritance pattern, meaning a child of an affected parent has a 50% chance of inheriting the mutation. Sporadic Fatal Insomnia (SFI), however, is not inherited and occurs without a family history.
Who should consider genetic testing for fatal insomnia?
Genetic testing is recommended for people with a family history of FFI or unexplained, rapidly progressive sleep disturbances combined with neurological symptoms. Genetic counseling is an important first step to understand the risks, benefits, and emotional implications of testing for the PRNP mutation.